MAY-GRÜNWALD GIEMSA STAIN
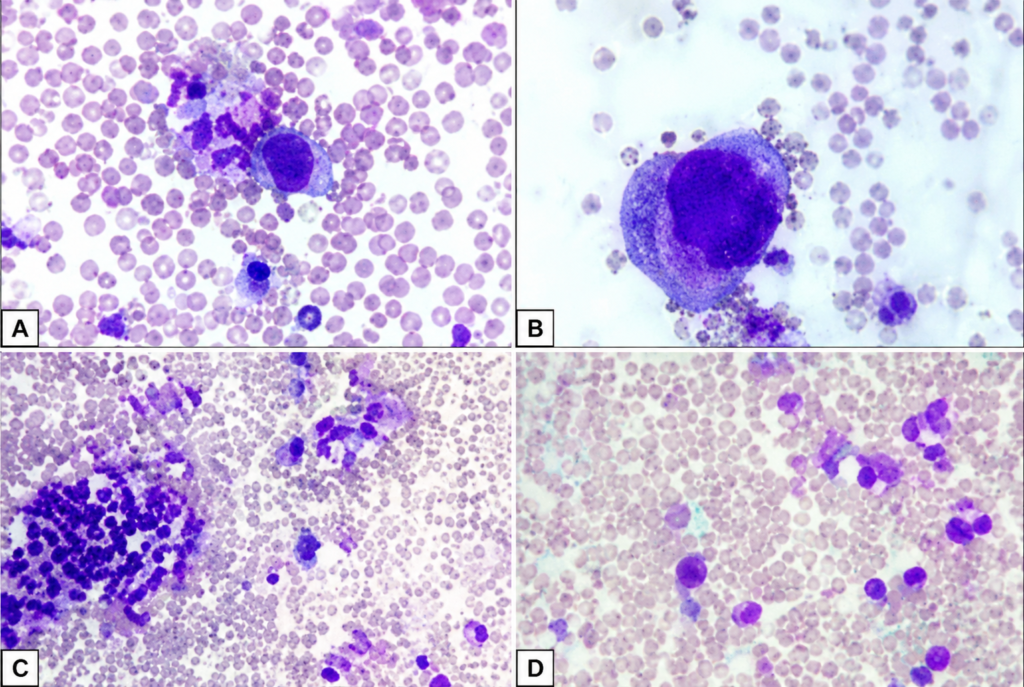
MAY-GRÜNWALD GIEMSA STAIN:- This is one of the common Romanwsky stains used in cytology. It is useful for studying cell morphology in air-dried smears. It is superior to Papanicolaou to study the cytoplasm, granules, vacuoles, basement membrane material etc. For nuclear staining Papanicolaou is superior. Contents of the staining reagents:- May-Grünwald solution 0.2% Methanol 99 %May-Grünwald´s eosin-methylene blue 0.2 % Contains:- Eosin G, Methylene blue Giemsa solution:- Methanol 73 % Glycerol 26 %Giemsa´s Azur-Eosin-Methylene blue 0.6 % Contains: Azur I, Eosin G, Methylene blue Phosphate buffer:- Potassium dihydrogen phosphate/ disodium hydrogen phosphate x 2H2O (67.0 mmol/l) Storage:- Giemsa solution, May-Grünwald solution: protected from light at 2-25°C.Unopened reagents may be used until the expiry date on the label.Phosphate buffer: at 2-8°C. Unopened reagents may be used until the expiry dateon the label. Preparation of working solutions:- 1. Buffered water: Dilute phosphate buffer with deionised or distilled water1:20, e.g. 30 ml phosphate buffer + 570 ml deionised or distilled water.2. Giemsa working solution : Mix 84 ml of Giemsa solution into 516 ml ofbuffered water.3. May-Grünwald working solution: Mix 360 ml of May-Grünwald solutioninto 240 ml of buffered water. Staining method:- 1. Fix the air-dried smear specimen in methanol for 10 -20 minutes2. Stain with May-Grünwald working solution for 5 minutes3. Stain with Giemsa working solution for 12 minutes4. Wash with clean buffered water for 2, 5 and 2 minutes5. Dry the slides in upright position at room temperature6. Mount the slides with a coverslip using DPXAny modifications to the staining procedure/working solutions may affect thestaining result, and are subject to precise method validation Sources of errors:- Irregular distribution of the blood smear on a glass slide may result in an erroneous cell counts. Alcohols used for wiping the skin may cause hemolysis and artifacts. Do not let the specimens dry at any stage of the staining procedure. Wash properly to avoid dye artifacts. Buffered water is strongly recommended for washing. Staining result is dependent on pH. Alkaline pH increases blue and acidic pH pink or reddish tinge in the stained specimen. Ziehl-Neelsen stain:- Reagents:- (1) Carbol Soft FuchsinBasic Fuchsin 1 gmAbsolute alcohol 10 mlAdd the basic fuchsin to the alcohol in a 100 ml flask and mix, on amagnetic stirrer for 30 minutes. Add 100ml of 5% aqueous phenol. Mixwell. Filter and store in a brown glass bottle. (2) Acidified Methylene Blue0.25% methylene blue in 1% acetic alcohol (3) 0.5% Acid AlcoholDistiller water 700 mlAbsolute alcohol 300 mlHydrochloric acid 5 ml (6) 5% Sulphuric AcidDistilled water 475 mlSulphuric acid 25 ml Staining Method:- Place fixed slides on the staining rack in serial order, smeared side up. Slides should be separated by a 1 cm gap, and should never touch one another. Cover slides individually with filtered Ziehl’s carbol fuchsin working solution. Heatslides from underneath with the flame of a Bunsen burner, an alcohol lamp or an alcohol soaked cotton swab until vapour starts to rise. Staining solution should never be allowed to boil. Do not allow the stain to dry. Keep slidescovered with hot, steaming carbolfuchsin for 5 minutes by re-flaming as needed. Rinse slides gently with water to remove excess carbolfuchsin. Drain off excess rinsing water from slides. Sputum smears appear red in colour. Decolourising: Cover slides with 25% sulfuric acid or acid-alcohol solution and allow to stand for 3 minutes, after which the red colour should have almost completely disappeared. If needed, repeat sequence until the red colour disappears, but do not overdecolourise. Gently wash away the sulfuric acid or acid alcohol and the excess stain with water. Drain off excess rinsing water from slides. Counterstaining: Cover slides individually with 0.3% methylene blue counterstaining solution and allow to stand for 1 minute. Rinse slides individually with water. Drain water off the slides, which are then allowed to air dry. A properly stained smear should show a light blue colour due to methylene blue. Results:- Tubercle bacilli, hair shafts, Actinomyces, some fungal elements- red. Background: pale blue.